Post-CABG Phase II Rehabilitation: Weeks 4–12 Protocol for Physiotherapy Students
Learn the Phase II post-CABG rehabilitation protocol for weeks 4–12, including FITT exercise prescription, beta-blocker target HR, return to work and psychosocial screening.
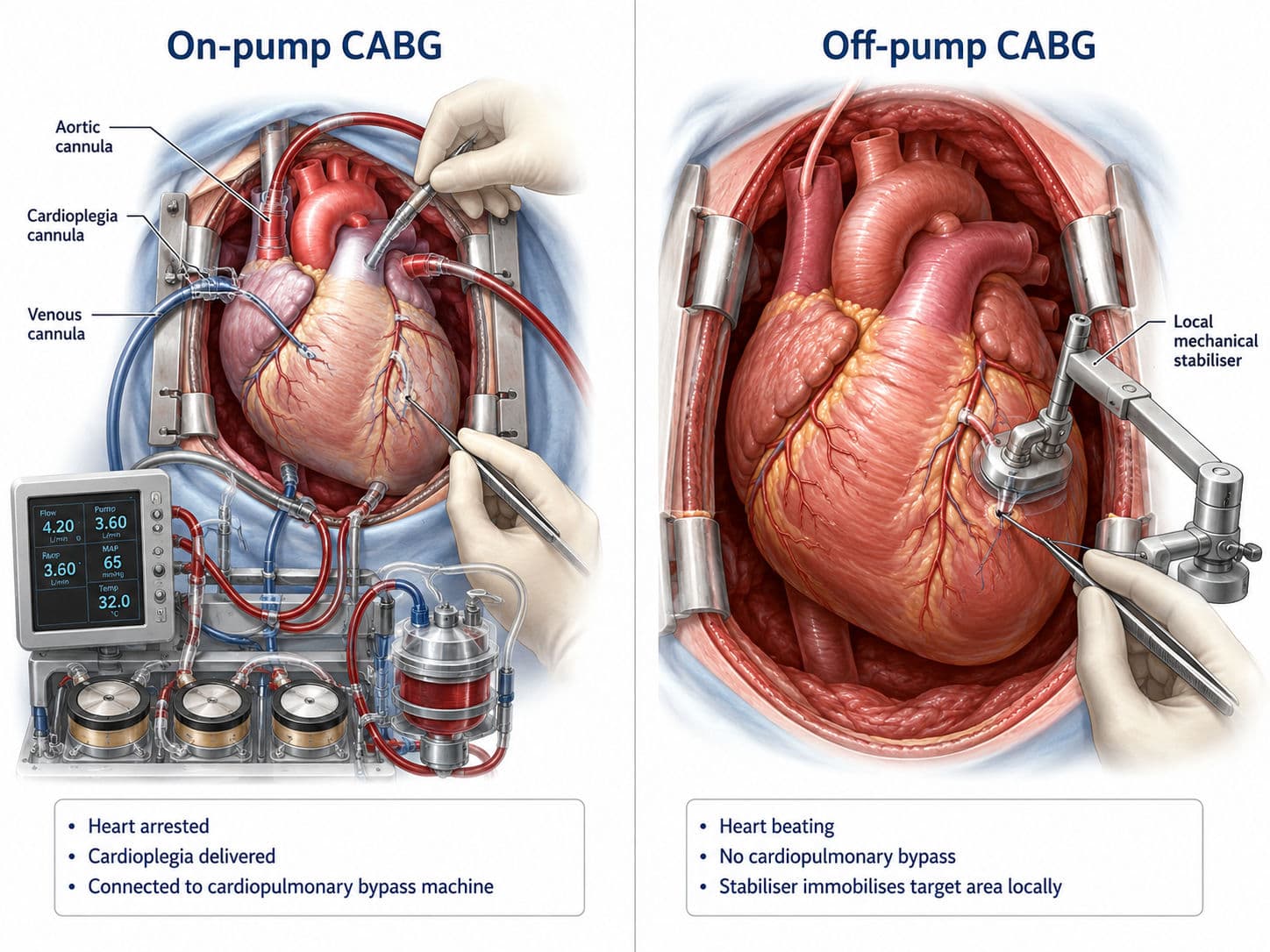
Coronary artery bypass grafting restores myocardial blood flow, but surgery alone does not correct the physical deconditioning, cardiovascular risk factors or fear of activity that frequently accompany coronary artery disease. Phase II cardiac rehabilitation bridges this gap through supervised exercise, risk-factor management, education and psychosocial support.
Although outpatient rehabilitation may begin earlier in selected stable patients, this article focuses on the clinically important weeks 4–12 after CABG, when walking capacity improves, the sternum continues to heal and patients begin returning to work and independent activity.
Phase II: From Surgical Recovery to Functional Independence
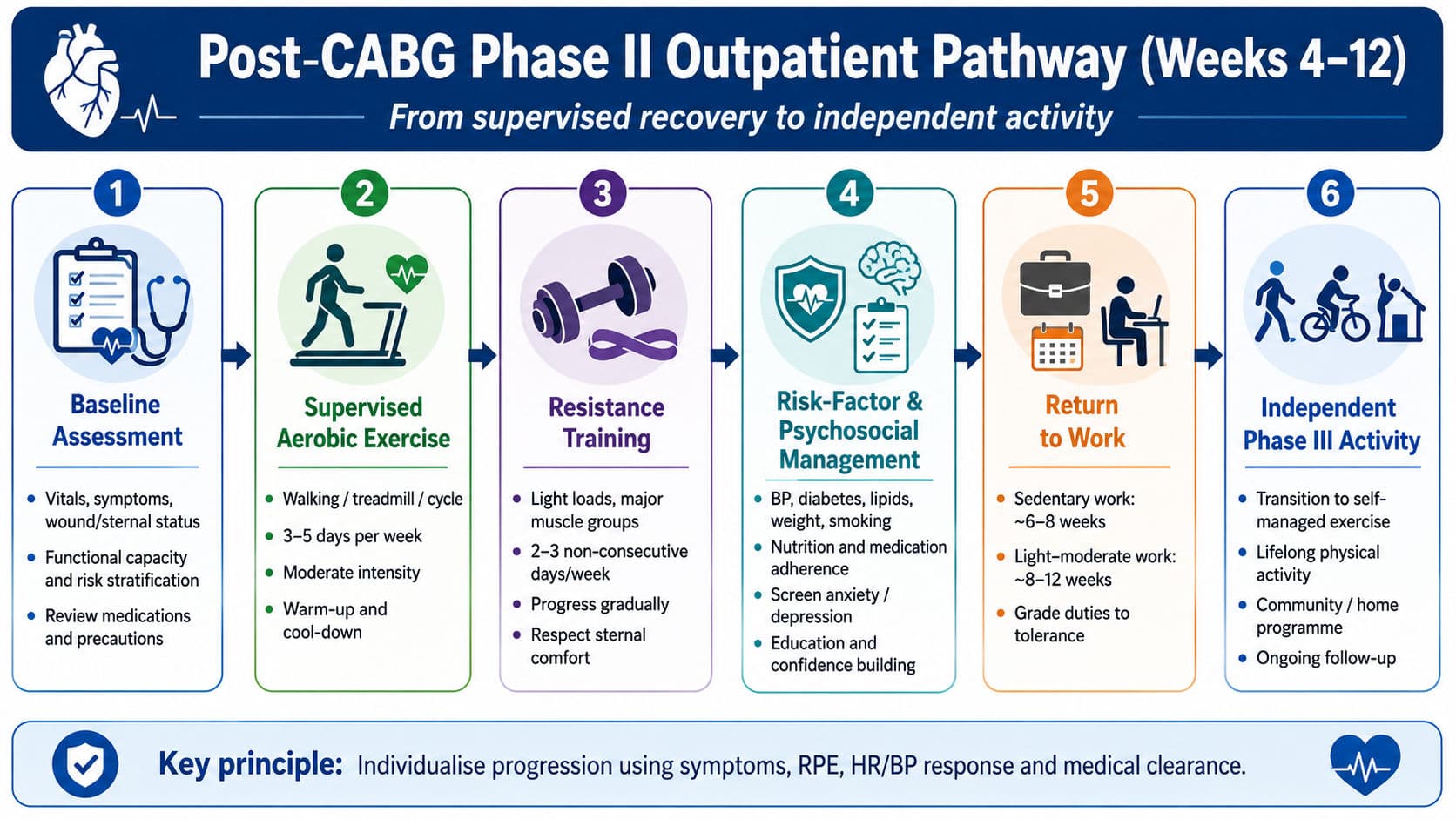
Phase II is a medically supervised outpatient programme that usually follows discharge and continues for approximately 8–12 weeks. Its purpose is not simply to “make the patient exercise". It aims to:
- restore functional and cardiorespiratory capacity;
- increase confidence during physical activity;
- identify abnormal exercise responses;
- control blood pressure, diabetes, lipids, weight and tobacco exposure;
- support medication adherence;
- address anxiety, depression and fear of recurrence; and
- prepare the patient for work, recreation and lifelong exercise.
The updated American Heart Association and American Association of Cardiovascular and Pulmonary Rehabilitation framework identifies patient assessment, aerobic training, strength training, physical activity counselling, psychosocial management, nutrition and cardiovascular risk factor control as core components of cardiac rehabilitation (Brown et al., 2024).
Clinical pearl: Phase II is not defined only by time after surgery. Entry depends on medical stability, wound healing, functional status and the absence of uncontrolled postoperative complications.
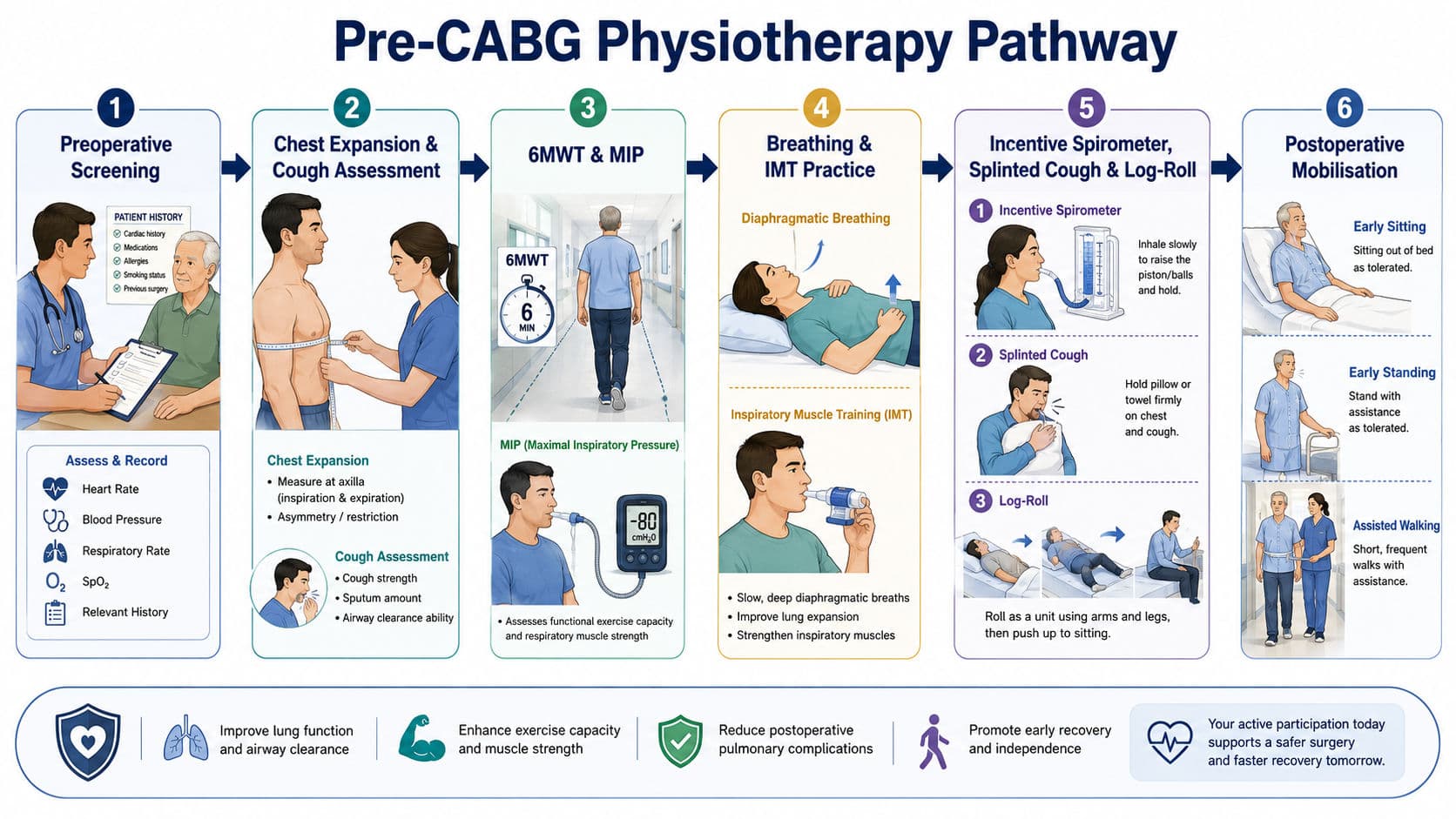
Assessment Before the First Exercise Session
The physiotherapist should first review the operative summary, postoperative complications, left ventricular function, ECG findings, graft-harvest site, medications and cardiologist or surgeon instructions.
The baseline assessment should include:
- resting heart rate, blood pressure, respiratory rate and oxygen saturation;
- symptoms of angina, dyspnoea, palpitations, dizziness and fatigue;
- sternal wound healing, pain, clicking or instability;
- lower-limb oedema and graft-harvest-site complications;
- postural blood-pressure response;
- glucose control in patients with diabetes;
- musculoskeletal limitations and balance;
- functional capacity using a symptom-limited exercise test, cardiopulmonary exercise test, six-minute walk test or incremental shuttle walk test;
- occupational and home demands; and
- depression, anxiety, sleep, cognition, social support and fear of movement.
AACVPR risk stratification classifies patients according to ventricular function, functional capacity, exercise-induced ischaemia, arrhythmias, symptoms and haemodynamic responses. Higher-risk patients require closer ECG and blood-pressure monitoring, slower progression and greater medical supervision (American Association of Cardiovascular and Pulmonary Rehabilitation [AACVPR], 2020).
Exercise should be deferred and the medical team informed when there is unstable angina, decompensated heart failure, uncontrolled arrhythmia, acute systemic illness, severe resting hypertension or hypotension, active wound infection, suspected sternal instability or another unstable postoperative complication.
FITT Exercise Prescription for Weeks 4–12
Exercise prescription must be based on the patient’s test results, medication response and surgical recovery rather than on the postoperative week alone.

Walking is usually the most accessible starting mode. Intervals such as three to five minutes of activity followed by brief active recovery may be used when continuous exercise is initially limited by fatigue. The aim is to gradually accumulate a clinically meaningful weekly aerobic volume rather than chasing speed during early sessions (Savage et al., 2025).
Resistance training improves strength, occupational capacity and independence. Carefully supervised earlier training may be appropriate in selected patients with stable wounds and surgeon clearance.
A conservative starting prescription is:
- one set of 10–15 repetitions;
- approximately 30%–40% of one-repetition maximum for the upper limbs;
- approximately 50%–60% for the lower limbs;
- slow, controlled movements;
- pain-free range;
- normal breathing without the Valsalva manoeuvre; and
- gradual progression to two or three sets.
Functional exercises may include sit-to-stand, heel raises, supported squats, light rowing movements and low-resistance upper-limb work. The load should remain close to the body, and pushing or pulling should stop if it produces sternal pain, clicking or instability.
Target Heart Rate Under Beta-Blockade
Beta-blockers reduce resting heart rate and blunt the heart-rate response to exercise. Therefore, formulas such as 220 − age may substantially misrepresent the patient’s actual maximum heart rate.
The preferred method is to use the peak heart rate obtained from a symptom-limited exercise test performed while the patient is taking the usual beta-blocker dose.
Target HR = Resting HR + Training fraction × (Measured peak HR − Resting HR)
For example, if resting HR is 62 beats/min and measured peak HR is 118 beats/min:
- HR reserve = 118 − 62 = 56 beats/min
- at 50% HR reserve: 62 + (0.50 × 56) = 90 beats/min
- at 70% HR reserve: 62 + (0.70 × 56) = 101 beats/min
The initial target zone would therefore be approximately 90–101 beats/min, provided symptoms, ECG and blood pressure responses are satisfactory.
When an exercise test is unavailable, RPE, the talk test, symptoms and haemodynamic response should guide intensity. Resting HR plus 20–30 beats/min may be used as a cautious temporary estimate, but it is not equivalent to a test-derived prescription and may underdose exercise. Research in beta-blocked cardiac-rehabilitation participants found that predicted maximum-heart-rate equations and simple resting-HR increments frequently failed to match target ranges calculated from measured peak heart rate (Keteyian et al., 2023).
Exam pearl: In a patient taking beta-blockers, prioritise measured exercise-test HR, RPE and clinical response—not age-predicted HRmax.
Progression, Safety and Return to Work
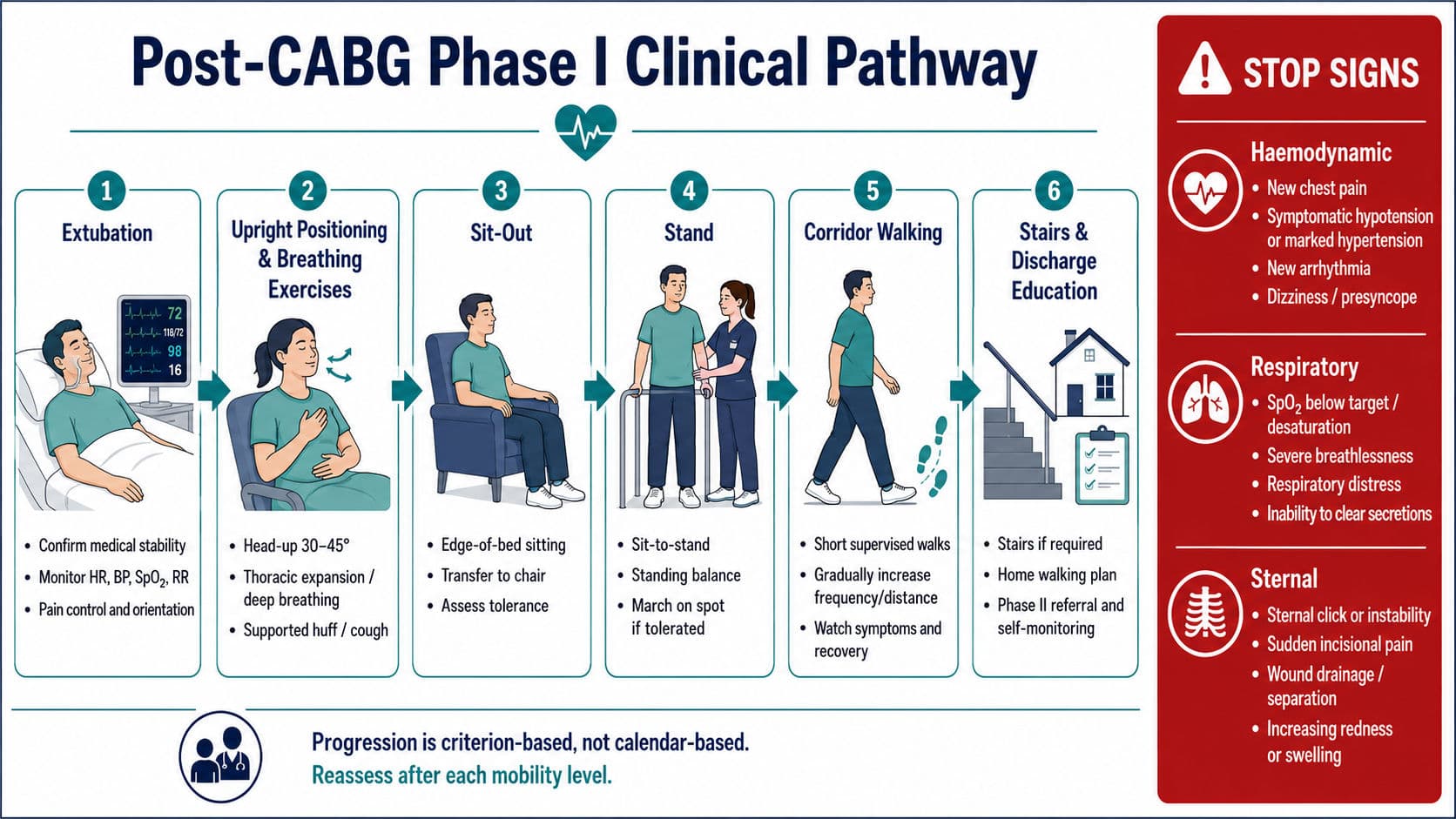
During early Phase II sessions, monitor heart rate, rhythm when indicated, blood pressure, RPE and symptoms before, during and after exercise. Progression may occur when the patient completes the prescribed duration without angina, excessive dyspnoea, abnormal fatigue or delayed recovery.
Exercise should be reduced or stopped when the patient develops:
- angina or angina-equivalent symptoms;
- dizziness, presyncope, confusion or marked pallor;
- disproportionate breathlessness;
- new or worsening arrhythmia;
- a fall in systolic blood pressure with increasing workload;
- an excessive hypertensive response;
- abnormal oxygen desaturation;
- new sternal pain, clicking or wound discharge; or
- unusual graft leg pain or swelling.
Return to work should be planned rather than decided solely by the calendar. Many uncomplicated patients performing sedentary work may return at approximately six to eight weeks, whereas light-to-moderate physical work may require eight to twelve weeks. Heavy manual work commonly requires at least 12 weeks, demonstrated functional capacity and explicit surgical or cardiology clearance.
The assessment should consider lifting, carrying, climbing, prolonged standing, shift work, driving, environmental heat and psychological stress. A graded return—such as shorter hours, lighter duties and planned rest breaks—is often more successful than immediate full-time resumption. Fatigue, poor sleep and reduced concentration may persist even when the sternum appears clinically healed.
Psychosocial Screening and the Indian Context
Anxiety, low mood, sleep disturbance, fear of exertion and concerns about graft failure are common after cardiac surgery. These factors can reduce participation even when the patient is physically capable of exercising.
Psychosocial assessment should occur at entry and again before discharge from Phase II. Useful validated instruments include the following:
- Patient Health Questionnaire-2 or PHQ-9 for depression;
- Generalized Anxiety Disorder-2 or GAD-7 for anxiety; and
- The Hospital Anxiety and Depression Scale was routinely used.
Screening should also explore social isolation, caregiver burden, financial stress, work insecurity, sexual concerns, cognitive changes, sleep and confidence in self-management. Positive findings require appropriate education, behavioural support or referral. Any indication of self-harm or suicidal thinking requires urgent medical and mental-health escalation.
The Cardiological Society of India position statement supports comprehensive, culturally sensitive cardiac rehabilitation incorporating exercise, education, risk-factor modification and psychosocial care (Cardiological Society of India, 2017). However, India does not currently have a widely adopted IACTS-specific exercise protocol for Phase II after CABG.
Indian cardiac-rehabilitation capacity remains limited relative to the burden of coronary disease (Babu et al., 2020). Practical delivery may therefore include supervised hospital sessions combined with home walking, telephone follow-up, digital monitoring, family education and low-cost resistance exercises. Hybrid care must still include documented assessment, individual prescription, symptom education and a clear escalation pathway.
Viva-Ready Summary
- Phase II is supervised outpatient cardiac rehabilitation focused on exercise, secondary prevention and return to participation.
- Prescribe exercise using FITT: aerobic training 3–5 days/week, initially at moderate intensity, progressing in duration before intensity.
- In beta-blocked patients, calculate target HR from a measured exercise test performed on usual medication.
- Add resistance exercise gradually after confirming wound and sternal stability.
- Return to work depends on functional capacity, job demands, healing and psychological readiness—not postoperative week alone.
- Screen every patient for depression, anxiety, sleep disturbance, fear of activity and social barriers.
One-line recall: Post-CABG Phase II uses test-based, symptom-monitored FITT exercise to rebuild capacity, control risk factors and restore confident participation in work and life.
References
American Association of Cardiovascular and Pulmonary Rehabilitation. (2020). Guidelines for cardiac rehabilitation and secondary prevention programmes (6th ed.). Human Kinetics.
American College of Sports Medicine. (2025). ACSM’s guidelines for exercise testing and prescription (12th ed.). Wolters Kluwer.
Babu, A. S., Turk-Adawi, K., Supervia, M., Lopez-Jimenez, F., Contractor, A., & Grace, S. L. (2020). Cardiac rehabilitation in India: Results from the International Council of Cardiovascular Prevention and Rehabilitation’s global audit of cardiac rehabilitation. Global Heart, 15(1), Article 28. https://doi.org/10.5334/gh.783
Brown, T. M., Pack, Q. R., Aberegg, E., Brewer, L. C., Ford, Y. R., Forman, D. E., Gathright, E. C., Khadanga, S., Ozemek, C., & Thomas, R. J. (2024). Core components of cardiac rehabilitation programmes: 2024 update: A scientific statement from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation, 150(18), e328–e347. https://doi.org/10.1161/CIR.0000000000001289
Cardiological Society of India. (2017). Cardiological Society of India: Position statement for the management of ST elevation myocardial infarction in India. Indian Heart Journal, 69, S63–S97. https://doi.org/10.1016/j.ihj.2017.03.006
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Keteyian, S. J., Steenson, K., Grimshaw, C., Mandel, N., Koester-Qualters, W., Berry, R., Kerrigan, D. J., Ehrman, J. K., Peterson, E. L., & Brawner, C. A. (2023). Among patients taking beta-adrenergic blockade therapy, use measured—not predicted—maximal heart rate to calculate a target heart rate for cardiac rehabilitation. Journal of Cardiopulmonary Rehabilitation and Prevention, 43(6), 427–432. https://doi.org/10.1097/HCR.0000000000000806
Savage, P. D., Beckie, T. M., Kaminsky, L. A., Lavie, C. J., & Ozemek, C. (2025). Volume of aerobic exercise to optimise outcomes in cardiac rehabilitation: An official statement from the American Association of Cardiovascular and Pulmonary Rehabilitation. Journal of Cardiopulmonary Rehabilitation and Prevention, 45(3), 161–168. https://doi.org/10.1097/HCR.0000000000000941