Post-CABG Phase I Rehabilitation: From ICU Day 1 to Discharge
A day-by-day Phase I physiotherapy protocol after CABG, covering positioning, breathing exercises, mobilisation milestones, sternal care and red flags that pause progression.
Phase I cardiac rehabilitation begins as soon as the patient is medically stable after coronary artery bypass grafting (CABG). Its purpose is not to “train” the patient in the conventional sense. It is to prevent avoidable complications, restore safe upright activity and prepare the patient for independent recovery after discharge.
Early mobilisation is now a central component of enhanced recovery after cardiac surgery. When appropriately screened and progressed, it can improve functional capacity at discharge without increasing adverse events (Grant et al., 2024; Kanejima et al., 2020). The protocol below is a practical framework; exact timing must follow the surgeon’s orders, haemodynamic status, lines and drains, comorbidities and institutional policy.
1. Start With Readiness, Not the Calendar
Before every session, review the operative notes, haemoglobin trend, rhythm, oxygen requirement, vasoactive support, chest-drain status, pain, cognition and recent clinical events. Confirm that the patient is responsive, able to follow commands and sufficiently stable for the proposed activity.
Record heart rate, rhythm, blood pressure, respiratory rate, oxygen saturation, symptoms and perceived exertion at rest. During early mobilisation, the target is usually light activity—approximately RPE 9–11 on the 6–20 Borg scale—rather than a fixed walking distance or heart-rate response. Beta-blockers, pacing, postoperative atrial fibrillation and autonomic changes may make heart rate alone unreliable (Hillegass, 2022).
A useful clinical rule is the following:
Assess → mobilise one level → reassess → progress only if recovery is satisfactory.
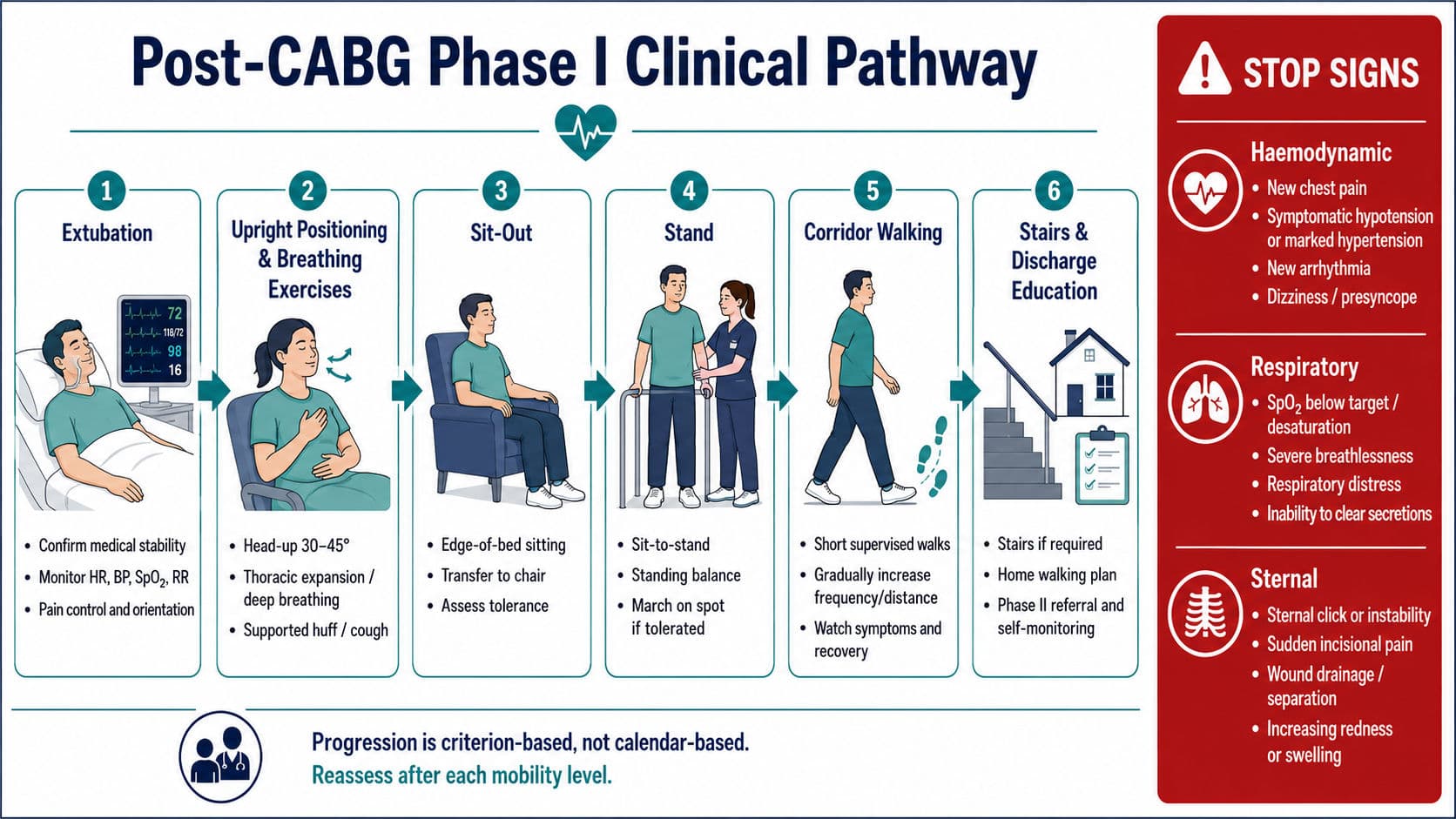
2. Extubation to Postoperative Day 1: Restore Ventilation and Upright Tolerance
After extubation, position the patient with the head of the bed elevated, commonly 30–45°, unless contraindicated. Regular turning, supported upright sitting and early chair positioning improve ventilation distribution and reduce the effects of prolonged supine lying.
Begin with:
- Breathing control and slow thoracic expansion exercises
- Supported huffing or coughing using a pillow or folded towel
- Ankle pumps and active lower-limb movements
- Gentle upper-limb movement within comfort and the prescribed sternal strategy
- Bed mobility using a log-roll or side-lying technique
- Sitting at the edge of the bed, followed by transfer to a chair when stable
When an incentive spirometer is prescribed, teach a slow, sustained inspiration rather than forceful blowing. It should support—not replace—deep breathing, coughing, positioning and mobilisation.
The first major milestone is sit-out of bed. The second is standing with assistance. Some stable patients may march on the spot or take a few steps on postoperative day 1; others may remain at chair level because of orthostatic intolerance, pain, bleeding risk or ongoing cardiovascular support. Progression is therefore criterion-based, not compulsory.
3. Postoperative Days 2–3: Stand, Transfer and Begin Corridor Walking
By postoperative day 2, the physiotherapist should aim to reduce assistance while preserving movement quality. Sessions may include repeated sit-to-stand practice, standing balance, marching, short corridor walks and active range-of-motion exercises. Walking is usually divided into several brief bouts rather than one fatiguing effort.
Monitor the patient before, during and after activity. Note symptoms, rhythm, blood pressure response, oxygen saturation, gait quality and the time required for values to return towards baseline. A patient who completes 20 metres comfortably may be safer to progress than one who completes 80 metres with marked breathlessness, dizziness or delayed recovery.
By postoperative day 3, suitable goals include:
- Supervised corridor ambulation two to four times daily
- Improving independence in bed mobility and transfers
- Completing basic self-care with pacing
- Practising controlled breathing during activity
- Reinforcing supported cough and wound awareness
Evidence supports early, structured mobilisation after cardiac surgery, but studies use different start times and exercise doses. Clinical stability and the response to the previous session therefore remain more important than rigid distance targets (Kanejima et al., 2020; Tazreean et al., 2022).
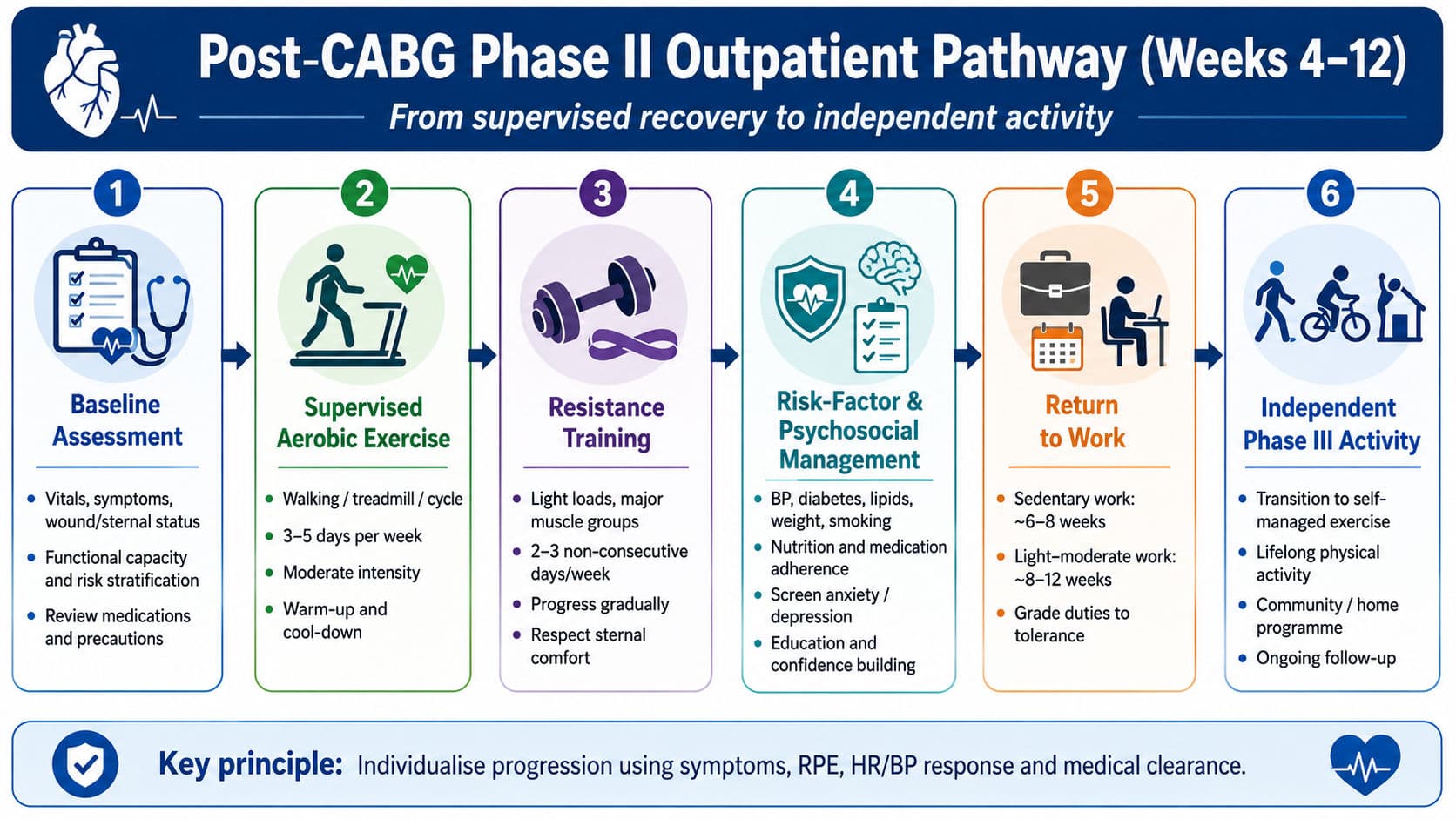
4. Postoperative Day 4 to Discharge: Build Independence, Not Exhaustion
During the step-down phase, walking distance, frequency and independence should increase gradually. The patient should be able to turn, transfer, use the toilet and walk on the ward with the least safe level of assistance. Stair assessment is added when required for the home environment and when lower-limb strength, balance and cardiovascular response are adequate.
Discharge preparation should cover:
- A progressive home-walking plan
- Pacing, rest breaks and the talk test
- Wound and sternal warning signs
- Safe coughing, rolling and sit-to-stand technique
- Medication adherence and risk-factor modification
- Enrolment in supervised Phase II cardiac rehabilitation
A successful Phase I is safe functional independence with clear self-monitoring skills and an organised transition to outpatient rehabilitation.
5. Breathing, Positioning and Sternal Protection: Clinical Pearls
Post-CABG breathing exercises should be purposeful. Use upright positioning, thoracic expansion, inspiratory holds when tolerated and supported airway clearance for patients with reduced expansion, retained secretions or an ineffective cough. Encourage frequent mobility because walking itself increases tidal ventilation and supports secretion clearance.
Pain management is part of respiratory physiotherapy. A patient who cannot inhale or cough because of pain needs reassessment and analgesic coordination, not repeated forceful instructions.
For sternotomy care, avoid pulling through one arm, forceful asymmetric pushing and sudden loaded reaching. A modern functional approach is to keep the upper arms close to the trunk—the “move in the tube” concept—and use pain, clicking or instability as warning signals. Less restrictive strategies may improve transfers and discharge independence without increasing sternal complications when applied appropriately (Born et al., 2025; Gach et al., 2021).
The pearl for students is simple: protect the sternum without making the patient afraid to move.
6. Red Flags That Pause Progression
Stop the activity, return the patient to a safe position and reassess when any of the following occurs.
Haemodynamic or cardiac red flags
- New or worsening angina-like chest pain
- Symptomatic hypotension, marked hypertension or a significant abnormal blood-pressure response
- New rapid, slow or complex arrhythmia
- Dizziness, presyncope, pallor, diaphoresis or sudden confusion
- Escalating vasopressor or inotropic requirement
- Acute heart-failure signs or poor peripheral perfusion
Respiratory red flags
- Oxygen saturation below the prescribed target, commonly below 90%, or a sustained fall despite support
- Severe or rapidly increasing breathlessness
- Respiratory rate below 5 or above 40 breaths/min
- New respiratory distress, cyanosis or inability to clear secretions
Sternal and surgical red flags
- New sternal clicking, shifting or visible instability
- Sudden sharp incisional pain during movement
- Wound separation, drainage, increasing redness or swelling
- Unexpected increase in chest-drain output, active bleeding or a surgeon-directed restriction
- Suspected deep sternal wound infection
Common screening thresholds such as resting heart rate below 40 or above 130 beats/min, systolic blood pressure below 90 or above 180 mmHg, or mean arterial pressure outside approximately 65–110 mmHg should be interpreted alongside symptoms, trends and medical orders—not used as isolated universal rules (Hodgson et al., 2014).
Post-CABG Phase I Protocol

Viva-ready summary
Phase I post-CABG rehabilitation is a monitored, criterion-based progression from positioning and breathing exercises to sit-out, standing, ambulation and discharge independence. The physiotherapist progresses activity only when haemodynamic, respiratory and sternal responses remain acceptable.
One-line recall point: After CABG, progress from breathe → sit → stand → walk → educate, but pause whenever the heart, lungs or sternum signal instability.
References
Born, R., Knott, K., Rea, A., Fonner, C. E., Roach, D., & Salenger, R. (2025). Replacing sternal precautions as part of a cardiac enhanced recovery program. Annals of Thoracic Surgery Short Reports, 3(2), 514–518. https://doi.org/10.1016/j.atssr.2024.10.015
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence to practice (6th ed.). Elsevier.
Gach, R., Triano, S., Ogola, G. O., da Graca, B., Shannon, J., El-Ansary, D., Bilbrey, T., Cortelli, M., & Adams, J. (2021). “Keep Your Move in the Tube” safely increases discharge home following cardiac surgery. PM&R, 13(12), 1321–1330. https://doi.org/10.1002/pmrj.12562
Grant, M. C., Crisafi, C., Alvarez, A., Arora, R. C., Brindle, M. E., Chatterjee, S., Ender, J., Fletcher, N., Gregory, A. J., Gunaydin, S., Jahangiri, M., Ljungqvist, O., Lobdell, K. W., Morton, V., Reddy, V. S., Salenger, R., Sander, M., Zarbock, A., & Engelman, D. T. (2024). Perioperative care in cardiac surgery: A joint consensus statement by the Enhanced Recovery After Surgery Cardiac Society, ERAS International Society, and the Society of Thoracic Surgeons. The Annals of Thoracic Surgery, 117(4), 669–689. https://doi.org/10.1016/j.athoracsur.2023.12.006
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Hodgson, C. L., Stiller, K., Needham, D. M., Tipping, C. J., Harrold, M., Baldwin, C. E., Bradley, S., Berney, S., Caruana, L. R., Elliott, D., Green, M., Haines, K., Higgins, A. M., Kaukonen, K.-M., Leditschke, I. A., Nickels, M. R., Paratz, J., Patman, S., Skinner, E. H., … Webb, S. A. (2014). Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Critical Care, 18, Article 658. https://doi.org/10.1186/s13054-014-0658-y
Kanejima, Y., Shimogai, T., Kitamura, M., Ishihara, K., & Izawa, K. P. (2020). Effect of early mobilization on physical function in patients after cardiac surgery: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 17(19), Article 7091. https://doi.org/10.3390/ijerph17197091
Tazreean, R., Nelson, G., & Twomey, R. (2022). Early mobilization in enhanced recovery after surgery pathways: Current evidence and recent advancements. Journal of Comparative Effectiveness Research, 11(2), 121–129. https://doi.org/10.2217/cer-2021-0258