How to Read PFTs: FEV1, FVC, GOLD Staging and Bedside Interpretation
Learn to interpret spirometry step by step: FEV1, FVC, obstructive and restrictive patterns, bronchodilator response, GOLD staging and loops.
Pulmonary function tests (PFTs) are a group of non-invasive tests used to assess how effectively the lungs move air, hold air and exchange gases. They include spirometry, lung-volume measurement and diffusion-capacity testing; however, this article focuses mainly on spirometry, the most commonly used component of PFT assessment.
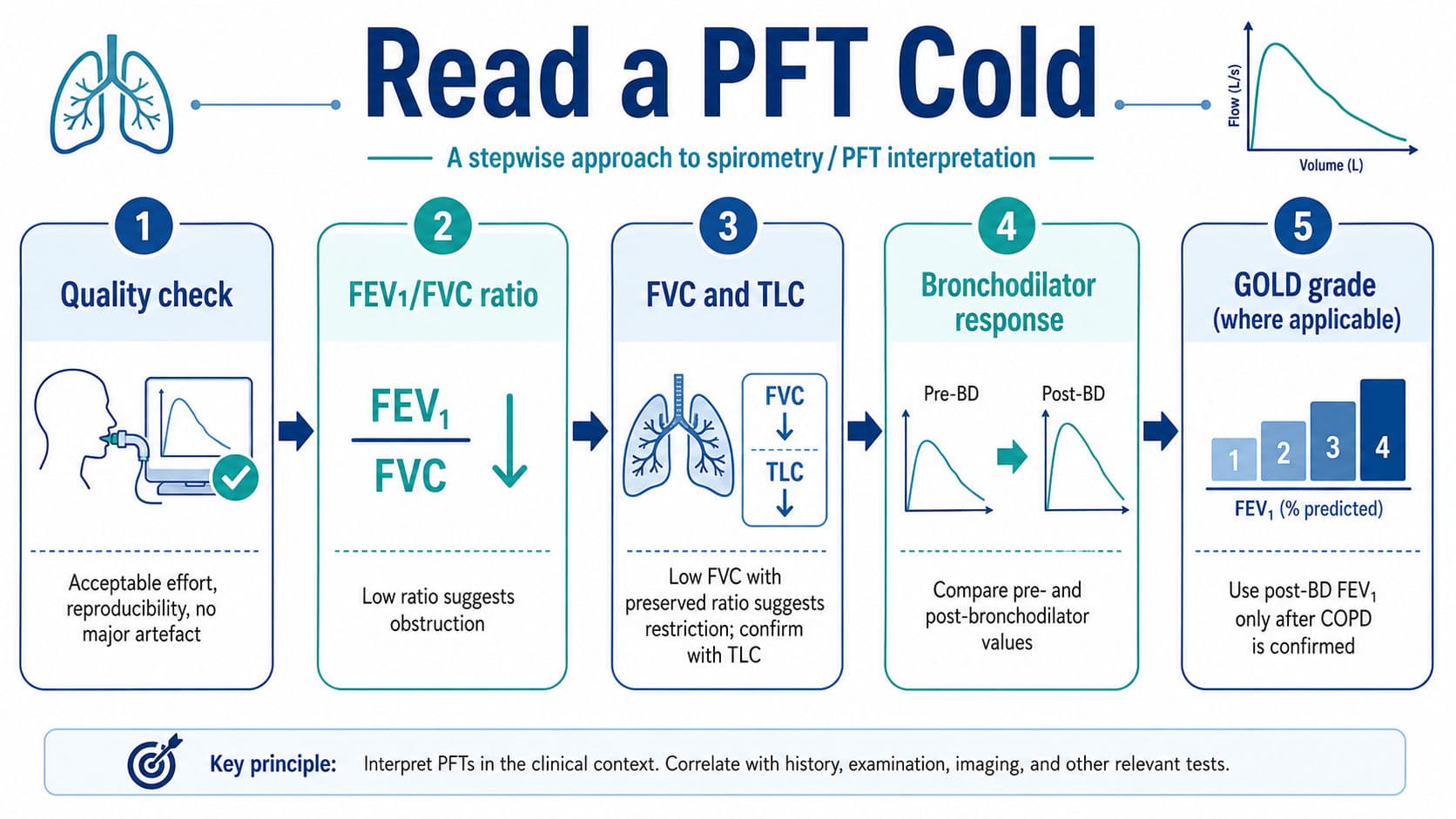
A pulmonary function test can look intimidating because a single report may contain litres, percentages, ratios, z-scores and two sets of values before and after a bronchodilator. The safest strategy is not to interpret every number at once. Read the report in a fixed order: check test quality, identify the ventilatory pattern, assess bronchodilator response and only then grade severity. This prevents the common mistake of calling a low FEV1 “obstruction” or a low FVC “restriction” without examining the ratio and lung volumes.
What Is Spirometry and How Is It Performed?
Spirometry is the most common pulmonary function test. It measures how much air you breathe in and out and how fast. Key values are FVC, FEV1 and the FEV1/FVC ratio. It helps detect airflow obstruction but cannot measure residual volume or total lung capacity.
For the forced vital capacity manoeuvre, the patient sits upright with a nose clip and seals the mouthpiece. They take a full breath in, then blow out as hard and fast as possible, keep blowing until empty, and finally breathe in fully again. The operator gives encouragement. Errors like coughing early, air leaks, poor seal or weak effort can affect results.
At least three attempts are needed. The best two FEV1 and FVC values should be within 150 mL. Stop once results are acceptable, usually within eight attempts.
Exam cue: Full breath in → blast out hard and fast → keep blowing until empty → breathe fully back in.
Know the Core Numbers Before Reading the Pattern
Forced vital capacity (FVC) is the total volume of air that a person can forcefully exhale after a maximal inspiration. Forced expiratory volume in one second (FEV1) is the portion exhaled during the first second. FEV1/FVC therefore reflects how rapidly the lungs can empty relative to the total forced exhaled volume.
The report usually shows the measured value, predicted value and percentage predicted. Predicted values account for factors such as age, sex and height. Contemporary interpretation preferably uses the lower limit of normal—or LLN—and z-scores rather than treating 80% predicted as a universal boundary (Quanjer et al., 2012; Stanojevic et al., 2022).

Before interpretation, look for an acceptable-quality or reproducible test. ATS/ERS standards generally require at least three acceptable manoeuvres, with the two largest FEV1 values and the two largest FVC values within 150 mL in adults (Graham et al., 2019). Cough, hesitation, poor mouth seal, submaximal inspiration or early termination can produce misleading results. A technically poor blow may imitate restriction.
Use a Fixed “Cold-Reading” Algorithm
Start with the measured FEV1/FVC ratio, not FEV1 alone.

For general PFT interpretation, the ratio should be compared with the age-appropriate LLN. For a GOLD diagnosis of COPD, however, persistent post-bronchodilator FEV1/FVC below 0.70 is the required spirometric criterion in the correct clinical setting (Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2026).
A low FVC does not confirm restriction because spirometry cannot measure residual volume or total lung capacity (TLC). Restriction is confirmed when TLC is below the LLN. In obstructive disease, FVC may also fall because air trapping prevents complete emptying during the forced manoeuvre.
The exam-ready sequence is:
Low ratio = obstruction. Low FVC with preserved ratio = suspect restriction. Low TLC = confirm restriction.
A true mixed ventilatory defect requires both a low FEV1/FVC ratio and a reduced TLC. Without lung-volume data, report the pattern cautiously rather than labelling it mixed.
Interpret Post-Bronchodilator Reversibility Correctly
Bronchodilator testing compares spirometry before and after an inhaled bronchodilator. The current ERS/ATS standard defines a significant response as a change in FEV1 or FVC greater than 10% of that individual’s predicted value (Stanojevic et al., 2022):
Bronchodilator response = (post-BD value − pre-BD value) ÷ predicted value × 100
Many university examinations and older reports still use the previous criterion: an increase in FEV1 or FVC of at least 12% and at least 200 mL from baseline. One should recognise both rules and clearly state which one they are applying.
A significant response supports variable airflow limitation, commonly seen in asthma, but it is not diagnostic by itself. Some patients with COPD demonstrate bronchodilator responsiveness, while a patient with asthma may show no significant response when clinically stable or already treated. The result must therefore be combined with symptoms, exposure history and previous variability.
For COPD, use the post-bronchodilator ratio to confirm persistent obstruction and the post-bronchodilator FEV1 percentage predicted for GOLD grading.
Apply GOLD 1–4 Only After COPD Is Confirmed
GOLD spirometric grades describe the severity of airflow obstruction in a patient who already meets the diagnostic criterion for COPD. They should not be applied to every obstructive spirometry report.

This is a grade of airflow limitation, not a complete statement of clinical severity. Dyspnoea, exercise tolerance, exacerbation history, oxygenation and comorbidities must be assessed separately (GOLD, 2026).
Reading the Flow-Volume Loop
The flow-volume loop provides a visual check of the numerical interpretation.
A normal expiratory limb rises rapidly to peak expiratory flow and then descends smoothly. In obstruction, peak flow is often reduced, and the expiratory limb becomes concave or “scooped out” because flow falls disproportionately at lower lung volumes.
A restrictive loop is smaller and narrower because the available lung volume is reduced, but its basic shape remains relatively preserved. The loop can suggest restriction, but TLC is still required for confirmation.
As an examination bonus, flattening of both inspiratory and expiratory limbs suggests fixed large-airway obstruction. Flattening predominantly during inspiration suggests variable extrathoracic obstruction, whereas expiratory flattening may indicate variable intrathoracic obstruction.

Worked Examples
Example 1: Obstruction with Significant Reversibility
The predicted FEV1 is 3.00 L. Pre-bronchodilator values are:
- FEV1: 1.80 L
- FVC: 3.40 L
- FEV1/FVC: 0.53
Post-bronchodilator FEV₁ is 2.18 L and FVC is 3.60 L.
The low pre-bronchodilator ratio shows obstruction. FEV1 improves by 0.38 L.
Using the current method:
0.38 ÷ 3.00 × 100 = 12.7% of predicted
This is a significant response. It also satisfies the older rule because the increase is 380 mL and approximately 21% from baseline.
Final interpretation: Obstructive ventilatory defect with significant bronchodilator response. Asthma becomes more likely, but clinical confirmation is still required.
Example 2: COPD with GOLD Grading
A smoker with chronic exertional dyspnoea has the following post-bronchodilator results:
- FEV1: 1.20 L
- Predicted FEV1: 2.80 L
- FVC: 2.50 L
- FEV1/FVC: 0.48
The post-bronchodilator ratio confirms persistent airflow obstruction.
FEV1 percentage predicted = 1.20 ÷ 2.80 × 100 = 42.9%
In the appropriate clinical context, this is COPD with GOLD 3 severe airflow limitation. Do not describe the entire disease as severe without also considering symptoms, exacerbations and functional limitations.
Example 3: Possible Restriction
The report shows:
- FEV1: 1.90 L or 68% predicted
- FVC: 2.20 L or 64% predicted
- FEV1/FVC: 0.86
Both volumes are low, but the ratio is preserved. Spirometry, therefore, suggests a possible restrictive pattern, not confirmed restriction.
If TLC is subsequently 65% predicted and below the LLN, restriction is confirmed. If TLC is normal, consider poor effort, air trapping, obesity-related respiratory mechanics or another nonspecific pattern.
Translate the Report into Bedside Physiotherapy Reasoning
PFTs describe respiratory mechanics; they do not replace bedside assessment. In obstructive disease, reduced expiratory flow may accompany prolonged expiration, dynamic hyperinflation and exertional breathlessness. The physiotherapist should relate the report to breathing pattern, inhaler technique, exercise-induced symptoms, secretion burden, oxygen saturation and functional capacity.
Pacing, interval training, breathing control and pulmonary rehabilitation may be relevant, but prescriptions should be based on the whole patient rather than FEV1 alone (Frownfelter et al., 2022; Hillegass, 2022). A bronchodilator-responsive pattern should also prompt review of inhaler technique, adherence and the timing of medication relative to exercise.
In a restrictive pattern, reduced lung volume may limit ventilatory reserve, and exertional desaturation can become clinically important. Monitor symptoms and SpO₂ during activity and consider whether the cause is parenchymal, pleural, neuromuscular, chest-wall-related or obesity-associated.
Viva-Ready Summary
- Read quality → FEV1/FVC → FVC → TLC → bronchodilator response → severity.
- A low FEV1/FVC ratio indicates obstruction.
- Low FVC with a preserved ratio only suggests restriction; low TLC confirms it.
- Current significant bronchodilator response is a rise in FEV1 or FVC greater than 10% of predicted.
- The older exam rule is an increase of at least 12% and 200 mL from baseline.
- GOLD 1–4 uses post-bronchodilator FEV1 percentage predicted only after COPD is confirmed.
One-line recall: The ratio identifies obstruction, TLC confirms restriction, reversibility tests variability, and post-BD FEV1 grades COPD.
References
Downie, P. A., Innocenti, D. M., & Jackson, S. E. (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Faber and Faber.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Elsevier.
Global Initiative for Chronic Obstructive Lung Disease. (2026). Global strategy for prevention, diagnosis and management of COPD: 2026 report.
Graham, B. L., Steenbruggen, I., Miller, M. R., Barjaktarevic, I. Z., Cooper, B. G., Hall, G. L., Hallstrand, T. S., Kaminsky, D. A., McCarthy, K., McCormack, M. C., Oropez, C. E., Rosenfeld, M., Stanojevic, S., Swanney, M. P., & Thompson, B. R. (2019). Standardization of spirometry 2019 update: An official American Thoracic Society and European Respiratory Society technical statement. American Journal of Respiratory and Critical Care Medicine, 200(8), e70–e88. doi:10.1164/rccm.201908-1590ST
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Quanjer, P. H., Stanojevic, S., Cole, T. J., Baur, X., Hall, G. L., Culver, B. H., Enright, P. L., Hankinson, J. L., Ip, M. S. M., Zheng, J., & Stocks, J. (2012). Multi-ethnic reference values for spirometry for the 3–95-year age range: The Global Lung Function 2012 equations. European Respiratory Journal, 40(6), 1324–1343. doi:10.1183/09031936.00080312
Stanojevic, S., Kaminsky, D. A., Miller, M. R., Thompson, B., Aliverti, A., Barjaktarevic, I., Cooper, B. G., Culver, B., Derom, E., Hall, G. L., Hallstrand, T. S., Leuppi, J. D., MacIntyre, N., McCormack, M., Rosenfeld, M., & Swenson, E. R. (2022). ERS/ATS technical standard on interpretive strategies for routine lung function tests. European Respiratory Journal, 60(1), Article 2101499. doi:10.1183/13993003.01499-2021